The Patient
Unit 7: Wound Healing & Management
Topic 4: Wound Management in Various Tissues
The basic processes of healing occur in all types of tissues with a number of variations characteristic of the tissue itself.
Selection of the appropriate sutures in repairing these tissues depends on not only a knowledge of the properties of the suture material, but also a thorough knowledge of the healing characteristics of the tissues and organs into which they are placed.
Foetal Tissue
The foetus responds to injury in a fashion that is remarkable and quite different to that of an adult. Foetal wounds heal rapidly and without the degree of scarring, inflammation or contraction seen in adults.
Epithelial and Endothelial Lined Tissues
A few general facts should be stated about basic wound healing in epithelial and endothelial lined tissues:
- The lining cells of hollow viscera (endothelium) and superficial cells of exposed surfaces
- (epithelium) are constantly being renewed. What happens after superficial injury is simply a variation of this theme;
- Regardless of the site, the process of epithelial mobilization, migration and mitosis are similar in the different tissues;
- Variations occur in full thickness wounds - the healing and contribution of surrounding and underlying tissues determine the type of healing that takes place;
- In general, smooth muscle associated with epithelial or endothelial surfaces, fails to regenerate and instead, heals by fibrous union.
Skin
Healing of the skin and migration of the epithelium have been detailed in Topic 2 of this Unit.
In an incised wound the advancing epithelium usually unites within 48 hours.
Further downward epithelial growth also occurs within the incision.
The epithelium gradually acquires structural features of the adjacent uninjured epidermis.
The development of keratin in the epithelial cells of the uppermost scar precedes loosening of the overlying scab which can usually be dislodged after 5 days.
In open wounds contraction also helps to close the wound.
In many domestic animal wounds, some degree of self-mutilation occurs (rubbing, biting, scratching, licking, trauma from bandage). This interferes with the normal orderly pattern of cell migration.Humans and horses have species-specific problems with open wound healing. Human skin can react in certain areas by deposition of excessive scar tissue and a poor epithelial covering (keloid).
Horses also can respond to open wounds by laying down excessive granulation tissue - Proud Flesh (see later).

Sutured skin wound

Simple interrupted sutures
Suture Types and Patterns for skin closure
Traditionally simple interrupted non-absorbable sutures have been used for the closure of skin wounds. Monofilament sutures such as 2/0 or 3/0 nylon and polypropylene are preferable to reduce the risk of wicking infection into the wound. The introduction of the monofilament absorbable materials (eg. PDS and Maxon) which retain their tensile strength for extended periods have also allowed their use in skin.

Cruciate suture
A variation on this is the cruciate suture pattern.

Interlocking suture
Continuous suture patterns are quicker to place than interrupted sutures, but rely entirely for their security on the knot at each end. A suture pattern frequently used for this purpose is the interlocking, or “blanket” suture.

Tight continuous skin suture
Skin sutures should produce accurate apposition of the wound edges without undue tension. Excessive tension will result in pressure necrosis of the skin under the suture due to compression of the local vascular (capillary) blood supply, and wound dehiscence.

Vertical mattress

Horizontal mattress
In thin skin and wounds under a mild degree of tension, everting techniques, such as horizontal mattress and vertical mattress sutures may be used. Slight eversion of the skin edges is preferable to inversion in respect to wound healing.
“Suture tracts” may form if significant injury has occurred whilst sutures were being placed in which epithelial cells grows down these tracts to produce unsightly scars. This can be avoided by using non-irritating, fine suture materials, and by removal of the sutures as early as possible.Wounds from which sutures are removed before the wound edges are stabilised by collagen, however, will have a weak scar which will widen. The skin edges may even separate. This may be avoided by the use of a buried subcuticular layer of absorbable sutures.
My personal preference is to use a continuous subcuticular layer of an absorbable monofilament such as Monocryl, PDS or Maxon. If performed carefully, no further external sutures are required, with a good cosmetic effect, and the subsequent healed wound is minimal.

Completed Subcuticular Suture

Subcuticular Suture

Click to view Video on Subcuticular Suture
Trachea
Tracheal epithelium has both goblet cells (secreting mucus) and ciliated cells. If injury involves the tracheal epithelium but does not involve the underlying supportive tissues, then tracheal epithelium healing will be complete.
If there is extensive loss of the underlying tissues, then scarring and poorly differentiated epithelium will cover the wound. Mucous may collect in these areas which have decreased ciliary activity leading to a chronic cough. There is also the potential that stricture of the lumen may occur exacerbating the decreased ability to clear mucous from the airways.
This follows one of the basic principles of epithelial healing:

Functional differentiation of epithelial cells is controlled by the nature of underlying structures.
To avoid this during tracheal surgery, only healthy tracheal tissues should be sutured accurately with absorbable sutures (4/0 or 5/0) minimizing exposure of the material to the lumen of the airways. Sutures placed around the tracheal or bronchial rings can be used to decrease tension across the sutured wound.

Sutured soft palate
Oral Cavity
Wounds of the oral mucosa are very quick to heal. This is no doubt due to the intense vascular supply of these tissues and their constant renewal as a result of natural sloughing.Rapidly absorbable sutures (size 3/0 or 4/0) are used in the oral cavity in either a simple interrupted or simple continuous suture pattern.

Damage to oesophagus

X-ray bone in oesophagus
Oesophagus
The epithelium of the oesophagus is stratified squamous but it is not keratinised. If only the epithelium is involved, complete wound healing is as expected. If deeper structures are involved, for example the damage resulting from foreign body obstruction and pressure necrosis, the subsequent fibrous tissue and scar formation can be extensive, and stricture is a common outcome.
The oesophagus does not have a serosa and thus this layer cannot be helpful in the prevention of leakage that commonly occurs from injuries in the alimentary tract.
Other factors that may decrease healing of oesophageal wounds include:
- the intramural blood supply may be affected in oesophageal resection / anastomosis;
- tension and motion due to the passage of food boluses;
- the lack of omentum (cf. rest of GIT);
- difficulty of exposure (particularly thoracic oesophagus);
- general debilitation of patients as a result of oesophageal problem;
- the oesophagus is commonly contaminated at the time of surgery.
Oesophageal closure
A multitude of suture techniques have been advocated for the oesophagus. The most widely recommended technique is a two-layer closure.
The first layer incorporates the mucosa/submucosa, and the second layer apposes the muscularis. A simple interrupted pattern is used. Simple continuous patterns can be used for eosophagotomy closures, but are not recommended for anastomoses because they impede oesophageal dilation. Traditionally it is believed that the holding layer of the oesophagus is the mucosa because of its thick stratified squamous epithelium. It has been recommended that 3/0 non-absorbable sutures be used with their knots tied in the lumen, where they can eventually be extruded.
It has been found however that the submucosa has the same tensile strength as the mucosa and submucosa together and with the advent of minimally reactive, slowly absorbable monofilament suture materials (PDS, Maxon), it is possible to use single-layer closures of 3-0 or 4-0 sutures that incorporate the submucosa and muscularis.
Stomach and Intestines
Healing properties
There are four types of epithelial cells in the stomach: mucus-secreting cells, parietal cells (produce HCI) and chief cells (produce pepsin), and simple columnar surface cells. When an injury occurs, the highly differentiated parietal and chief cells appear to undergo de-differentiation to mucus-secreting cells. When repair is complete, such cells appear to revert back to their normal secretory functions.
The removal of large areas of the stomach is possible without significant renewal of stomach size or contraction problems.
The small intestine has a rich blood supply with extensive collateral circulation. This enables the intestine to heal rapidly.
In the small intestine, normal continuous mitosis in the crypts between intestinal villi ensure constant renewal of villi cells every day (in humans, complete renewal of duodenal epithelium : 2.25 days; ileum: 2.75 days). After injury to small intestine epithelium, mitosis of crypt cells is followed by migration of these cells across the wound. Pre-existing cells do not migrate.
Significant problems occur in circumferential intestinal wounds due to stricture formation. This becomes particularly important when the surgeon is deciding on the appropriate type of suture material and pattern to use during intestinal resection/anastomosis.
Suture materials
A wide range of absorbable and non-absorbable materials have been used successfully in gastro-intestinal surgery.
Non-absorbable materials -
Historically, silk was used frequently without problems and has good handling properties. However due to its braided nature it should not be used in contaminated wounds due to its wicking effect. Better materials are available.
Polypropylene is an excellent material for use in contaminated wounds due to its monofilament nature. It is inert and has little tissue drag, however as the gastrointestinal tract heals rapidly, the indications for the use of non-absorbable sutures is limited.
Absorbable materials -
Catgut causes a greater tissue reaction than the synthetic materials. It is absorbed by enzymatic digestion and rapidly looses tensile strength in the presence of gastrointestinal enzymes, particularly in the stomach.
Dexon (polyglycolic acid) and Vicryl (polyglactin 910) are much less reactive. They are absorbed by hydrolysis of the material. Unless coated they will however create tissue drag and damage delicate tissues.
Polydioxinone (PDS-Ethicon) is a newer monofilament absorbable material which has better knot security, less tissue friction and is also absorbed by hydrolysis. it is very useful in contaminated areas.
Suturing gut
Polyglecapione 25 (Monocryl) is a monofilament absorbable suture which causes little tissue drag. It loses all effective tensile strength within three weeks, but is adequate for most intestinal use.
Generally 3/0 or 4/0 materials are best for intestinal sutures in small animals. A swaged on needle is preferable to minimize damage to the bowel wall.
All sutures must penetrate the submucosa - this is a basic surgical principle for suturing in the gastrointestinal tract, as it is the only layer with sufficient collagen to produce any real holding power.
Intestinal anastomoses are best begun at the mesenteric border because it has no serosal covering and sutures must be placed accurately to prevent leakage.

Stapler in use
A wide variety of stapling instruments are now on the market for gastrointestinal use. These are not used commonly in small animal surgery due to their high cost.
Intestinal Suture patterns
Suture patterns include end-to-end, end-to-side and side-to-side techniques. Most resections can be repaired using the end-to-end technique. The other patterns generally take longer to perform and are usually reserved for special areas such as gastroenterostomy or cholocystoenterostomy.
There are 3 main types of suture patterns:
- Inverting
- Everting
- Approximating

Inverted sutured gut
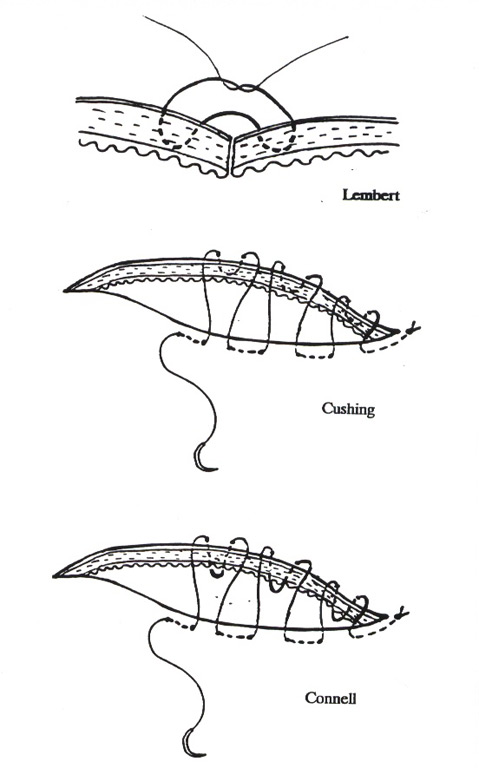
Lembert, Cushing, Connell
(1) Inverting patterns
This pattern produces serosa to serosa contact. This results in a rapid seal due to fibrin deposition across the serosal surfaces.
The classical technique is the 2-layer inverting technique of a primary Cushing or Connell layer followed by interrupted or continuous Lambert sutures.
Single layered closures are often used to reduce luminal narrowing.
(2) Everting pattern
This usually involves horizontal mattress sutures to evert all layers of the intestinal wall. It is easy to perform as the cut ends naturally evert, however the seal is very poor and the exposed mucosa may induce adhesions and excessive fibrosis resulting in narrowing of the lumen.
Drawing:simple interupted gut suture
(3) Approximating patterns
This pattern more accurately realigns the cut layers.
Three types of sutures can be used to achieve this:
- Simple interrupted non-crushing sutures.
Drawing: Cutting suture
(ii) Cutting sutures - these simple interrupted sutures are tied so that they cut through the mucosa, serosal and muscularis layers to just hold the submucosa in apposition.

Drawing: gambee suture
(iii) Gambee sutures - these penetrate the lumen and pass through the small segment of mucosa and submucosa on the same side increasing the strength of the suture. This also helps in pulling the mucosa back into the lumen of the bowel. The modified Gambee suture achieves a similar apposition of the bowel layers.
A comparison of healing, tensile strength and changes in luminal diameter is made in the table below.
|
Inverting Pattern |
Everting Pattern |
Approximating Pattern |
Intestinal Healing |
Inverted mucosa becomes necrotic and sloughs. Individual wall layers do not reform. |
Mucosa between sutures necroses. Healing process slower than others and inflammation greater. Adhesions much more likely. |
Healing is faster with less fibrous connective tissue layed down than other patterns. |
Tensile strength |
|
|
|
Post-operative luminal diameter
|
54-39% narrower |
3% narrower - but became the narrowest when healing complete. |
4% narrower |
It is apparent that there is little to recommend the everting pattern. The approximating pattern is becoming more popular due to its ease of operation, its maintenance of luminal diameter and rapid mucosal regeneration.
Simple interrupted non-crushing sutures are preferred over the crushing pattern because they cause less tissue necrosis and blood vessel disruption. Burst strengths and histological evaluations however show them to be similar when healed.
Everted mucosa can easily be trimmed with scissors to create a level surface for easier suturing.
Drawing: Continuous gut suture
Experienced surgeons may use a simple continuous suture pattern in the small intestine. Care must be taken not to cause constriction of the lumen with these sutures. Stay sutures are frequently placed at 180o can be useful in preventing this.
Large Intestine

Large intestine blood supply
Large intestine heals in a similar fashion to small intestine, but at a slower rate. The anatomy of the large intestine also differs from the small intestine in regard to its blood supply.

Sutured large intestine
nterrupted sutures of 3/0 or 4/0 monofilamant absorbable sutures are recommended.
Liver
Liver can regenerate nearly completely, even after 70% resection (experiments done in dogs). Unlike other tissues, where only the area immediately adjacent to the injury / resection site is involved in regeneration, in the liver, the whole remaining segment becomes involved.
Urinary Tract
A strong water-tight closure of the urinary bladder is desirable. Traditionally the bladder is closed with a 2-layered inverting technique, such as a continuous Cushing suture followed by a Lembert suture. The purpose of this is to achieve a serosa-to-serosa contact which is thought to produce a rapid seal. It has now been shown, however that there are no advantages of this technique, in regard to tensile strength, over a simple interrupted appositional closure.
Whilst the bladder heals quickly, the rapid loss of tensile strength of the multifilament absorbable sutures in the presence of alkaline urine and in particular infected urine has now been well demonstrated. These materials have, however, been used for many years in the bladder with few difficulties.
Suturing Bladder
Non-absorbable sutures should be avoided due the risk of them acting as a nidus of infection or calculus formation.
Peritoneum
The peritoneum is a single layer of squamous cells of mesothelial origin. It is so easily damaged that it tends to slough even after exposure to air or saline.
Regeneration is rapid and complete reperitonealization usually takes about 5-7 days. This begins within hours of an injury. Such rapid healing that is not dependent on the size of the defect and occurs through the differentiation of cells (eg. monocytes/fibroblasts) lying underneath the peritoneum.
Adhesions are a severe and common problem as a result of wound healing in the peritoneal cavity. They do not result every time the peritoneum in damaged by only when such damage is accompanied by the presence of:
- bacteria;
- devitalised tissue;
- foreign materials (including suture material).
Adhesions can obviously also form between structures contained in the peritoneal cavity eg. pieces of intestine. They can have disastrous consequences if they strangulate gut.
Some adhesions are very useful in the abdominal cavity eg. in the stoppage of leakage of gut contents.
If some sort of adhesion is required eg. around an anastomotic site, without the more serious consequences of `normal' adhesions, then it is suggested that omentum ("the abdominal policeman") can be wrapped around the site and sutured loosely into place. Alternatively, it can be expected that omentum will travel to the site of injury and cause a `natural' adhesion anyway.

Closing linea alba
Linea Alba and Fascia
The traditional way of closing the linea alba is by a simple interrupted pattern of either absorbable or non-absorbable material. The advent of the newer monofilament synthetic absorbable materials which retain their tensile strength for a prolonged period has allowed the safe use of continuous sutures for the closure of the abdomen. The introduction of the Maxon looped suture has further facilitated this time saving technique, although this suture relies entirely on the looped end to remain intact.
 Linea alba Closure
Linea alba ClosureIncisions in the linea alba frequently extend into the rectus fascia, particularly caudal to the umbilicus. These wounds are closed by suturing of the external rectus fascia only without inclusion of the rectus muscle or peritoneum. Studies have shown that inclusion of the peritoneum can increase the incidence of adhesions.
Nerves
Once the adult nervous system is fully developed, the capacity for mitosis (and hence regeneration) of nervous tissue is lost. Remaining cells can only repair themselves if their axons are intact.
Mild injury with no obvious physical disturbance to nerves is called neuropraxia - recovery occurs within 21 days.
If physical disruption to axons occur but Schwann cells and connective tissue remain intact (axonotmesis) there will be incomplete neurological deficits distal to injury. Complete severance of neural and connective tissue (neurotmesis) will result in total functional loss to regions distal to injury.
Apposing ends of nerves may not be sufficient for the complete restoration of function of nerves, as each nerve fibre within a bundle is a separate unit. Simply suturing the connective tissue surrounding the nerve bundle may not be sufficient to allow individual nerve fibre ends to `meet up with its' mate'.
Skeletal Muscle
If the injury is severe the muscle ends retract, leaving scar tissue to fill the gap.
If the injury is less severe or the muscle ends are united by suturing, histiocytes will remove devitalised tissue and sarcoplasm. By the 10th day nuclei accumulate at the rounded edges of the muscle and budding begins on either side of the cut. These may unite, but usually follow an irregular course.
Articular Cartilage
Articular cartilage has a very limited ability to heal. Partial thickness defects attempt to heal by the flow of cartilage matrix into the defect. Full; thickness defects heal by the influx of undifferentiated cells from defects which penetrate the subchondral bone. This will form fibrocartilage on the joint surface.
Bone
Bone heals in the same way as any wound and differs only in the maturation phase following the deposition of the granulation tissue bed.
The type of healing which subsequently occurs will depend principally on the degree of stability and immobilisation of the fracture site. An adequately stabilized wound (often achieved with the use of bone plates, external fixateurs or pins will result in the conversion of mesenchymal cells into osteoblasts and bone deposition.
Inadequate stabilization will result in the transformation of mesenchymal cells into chondroblasts and the deposition of fibrocartilage into the fracture site. This will result in a “non-union”. In response to this, the bone ends deposit additional periosteal new bone and a so-called hypertrophic non-union develops.
X-ray of non-union X-ray of healing bone
Tendon
Healing of tendon injuries is very complex. If we could rely on tendons healing in isolation to all other tissues surrounding them, then tendon healing would be greatly simplified.
Tendons do not possess sufficient cells to synthesise fibrous protein. Most of the cells in tendons (tenocytes) are probably inactive fibrocytes which do not have much capacity to `turn on' even after tendon injury. Indeed, tendon injuries that are isolated from surrounding tissues (eg. within tendon sheaths) are characterised by atrophy and resorption of the tendon ends. Therefore, regeneration of tendons has to depend on externally derived cells.
Fibroblasts from surrounding connective tissue migrate into the space between the tendon ends. Such cells excrete proteoglycans and collagen into the intercellular space, leading eventually to a dense fibrous scar. Adhesions extending from the tendon to surrounding tissues will occur. It is usually for the scar in association with the tendon ends will reform to some degree and subsequent collagen will realign longitudinally with the tendon. Such scar and collagen is never as strong as the original tendon and will be a potential site for further trauma.
In humans, restoration of tendon function is mainly assessed by the return of gliding function to the tendon (most tendon injuries in humans occur in the hand). In veterinary practice where patients are four-legged, adequate return of function is determined not only by adequate gliding function but also by the return to a strength that is capable of maintaining gait at the walk and during exercise.
A time-frame for tendon repair
- Week 4: Tendon ends `joined' by a fibrovascular mass that is not interdigitating with the tendon ends.
There is virtually no mechanical strength in such a wound.
- Week 8: Cellularity of wound is decreasing and there is some interdigitating with the tendon ends. There is still minimal strength.
- Week 8 - 12: Strength of area increases dramatically
- Week 24: Wound has mature characteristics.
Sutures used in the repair of tendons are usually non-absorbable and are placed in a pattern which directs the pull of the suture away from a longitudinal orientation. Monofilament suture materials such as nylon, polypropylene and stainless steel are preferred, although the newer longer-lasting monofilament absorbable sutures have been advocated as suitable for tendon repair.
Bunnell sutures aim to distribute the tension over a length of the tendon.
Modified Kessler sutures rely on the circumferential compression of part of the tendon to provide strength.
Additional support for the healing tendon such as splints and trans-articular stabilization devices such as screw and pins can help in the first few weeks to maintain proximity of the tendon ends. Weight bearing too early in the course of healing can result in stretching of the healing tendon and a subsequent loss of support to the affected limb.
 Transarticular pin
Transarticular pin  Sutured tendon
Sutured tendon  Lacerated tendon
Lacerated tendon  Drawing Tendon Sutures
Drawing Tendon Sutures